

Can a Simple CBC Predict Future Dementia Risk?
- David Stephen Klein, MD FACA FACPM

- 3 days ago
- 5 min read
The Monocyte-to-Lymphocyte Ratio and Its Emerging Role in Cognitive Decline.
One of the cheapest test that is currently available.

Quick Look
Could a routine complete blood count reveal early warning signs of future dementia?
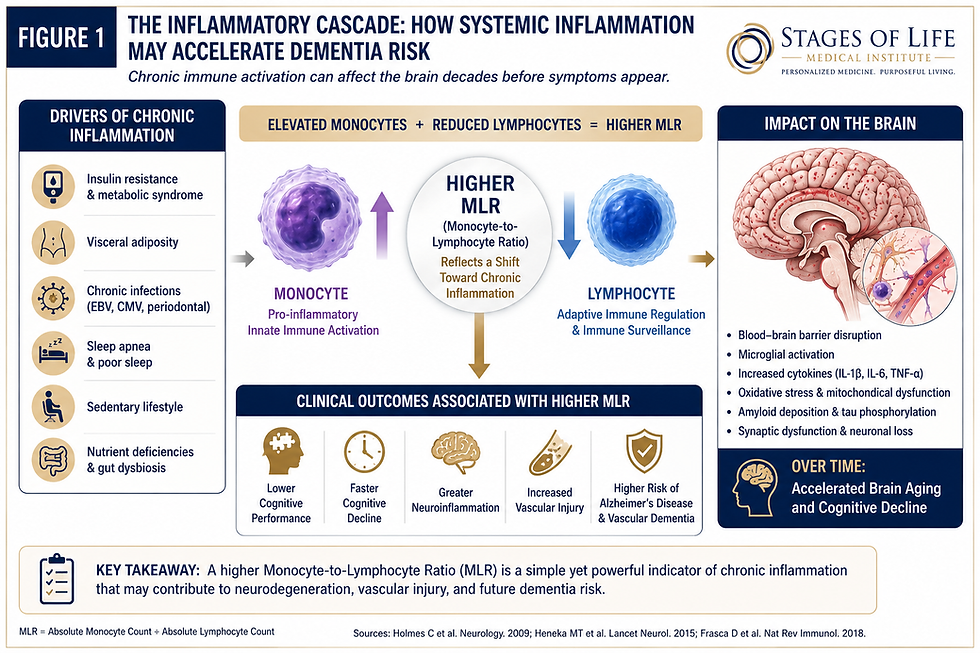
A growing body of evidence suggests that the monocyte-to-lymphocyte ratio (MLR) — a simple calculation derived from the CBC differential — may serve as a powerful marker of systemic inflammation, immune dysregulation, vascular injury, and accelerated brain aging. Elevated MLR levels have now been associated with increased neuroinflammation, amyloid accumulation, microglial activation, and poorer cognitive outcomes in patients at risk for Alzheimer’s disease and vascular dementia. Long before memory loss develops, subtle immune dysfunction may already be accelerating neurologic decline.
Inflammation: The Common Denominator of Aging
One of the major shifts in modern medicine has been the growing recognition that chronic low-grade inflammation plays a central role in aging.
Researchers now use the term “inflammaging” to describe persistent immune activation that slowly damages tissues over decades.
This process contributes to:
The challenge has always been finding inexpensive biomarkers capable of identifying this inflammatory burden early.
Interestingly, one of those markers may already be hiding in a routine CBC.
What Is the Monocyte-to-Lymphocyte Ratio?
The monocyte-to-lymphocyte ratio is calculated using two values from the white blood cell differential.
The Monocyte-to-Lymphocyte Ratio (MLR) is derived directly from a standard Complete Blood Count (CBC) with differential.
It compares two important white blood cell populations:
Monocytes → markers of innate immune activation and chronic inflammatory signaling
Lymphocytes → markers of adaptive immune regulation and physiologic resilience
The calculation is simple:
MLR = Absolute Monocyte Count ÷ Absolute Lymphocyte Count
Using a standard CBC:
CBC Differential | Value |
Absolute Monocyte Count | 0.72 K/µL |
Absolute Lymphocyte Count | 1.40 K/µL |
Calculation
Absolute Monocyte count divided by the Absolute Lymphocyte Count = MLR
Example:
Monocytes: 0.72 ×10⁹/L [0.72]
Lymphocytes: 1.40 ×10⁹/L [1.40]
0.72/1.40 = 0.51 (MLR)
The significance lies in what these cells represent biologically.
Quick office interpretation
MLR Result | Clinical Interpretation |
< 0.25 | Low inflammatory burden |
0.25 – 0.35 | Mild immune activation |
0.35 – 0.50 | Moderate chronic inflammation |
> 0.50 | Elevated inflammatory burden; possible accelerated biologic aging |
Monocytes represent:
Innate immune activation
Cytokine production
Chronic inflammatory signaling
Macrophage activation
Endothelial injury
Lymphocytes represent:
Adaptive immune regulation
Immune surveillance
Cellular resilience
Balanced inflammatory control
When monocytes rise relative to lymphocytes, the body often exists in a state of persistent inflammatory activation.
How Does This Affect the Brain?
The brain is extraordinarily sensitive to chronic inflammation.
Elevated MLR appears to correlate with several important neurologic processes.
1. Microglial Activation
Microglia serve as the brain’s resident immune cells.
Persistent systemic inflammation causes chronic activation resulting in:
Synaptic damage
Excess glutamate release
Oxidative stress
Increased neuronal death
2. Blood Brain Barrier Dysfunction
Inflammatory cytokines released by activated monocytes can weaken the blood brain barrier.
This allows inflammatory mediators access to vulnerable neural tissue.
3. Accelerated Amyloid and Tau Deposition
Studies suggest inflammatory signaling accelerates:
Beta amyloid plaque formation
Tau protein hyperphosphorylation
Mitochondrial dysfunction
All recognized features of Alzheimer's disease.

Clinical Pearl
One of the most overlooked concepts in cognitive medicine is that dementia begins biologically decades before memory loss begins clinically. Inflammatory biomarkers such as MLR may allow physicians to identify accelerated neurologic aging long before symptoms become obvious. By the time cognitive decline becomes clinically measurable, much of the damage may already be established.
Monitoring inflammatory markers early may permit intervention while the brain remains highly salvageable.
The Vascular Connection
Not all dementia begins with amyloid. Elevated inflammatory ratios strongly correlate with vascular injury.
High MLR levels are associated with:
Endothelial dysfunction
Increased platelet activation
Microvascular ischemia
Cerebral small vessel disease
Carotid plaque progression
Reduced nitric oxide signaling
This directly contributes to Vascular dementia. Many patients diagnosed with Alzheimer’s disease likely have mixed inflammatory and vascular mechanisms occurring simultaneously.
Proposed Reference Ranges
Although MLR is not yet standardized clinically, observational studies suggest useful ranges.
MLR | Interpretation |
0.15 – 0.25 | Lower inflammatory burden |
0.25 – 0.35 | Mild immune activation |
0.35 – 0.50 | Moderate chronic inflammation |
>0.50 | Elevated inflammatory burden |
Values should always be interpreted within clinical context.

What Causes Elevated MLR?
An elevated ratio often reflects underlying metabolic stress.
Common contributors include:
Insulin resistance
Hyperinsulinemia
Visceral adiposity
Chronic periodontal disease
Sleep apnea
Chronic viral activation (EBV, CMV)
Sedentary behavior
Metabolic syndrome
Autoimmune disease
Persistent gut dysbiosis
Importantly, these same conditions also accelerate biologic aging.
A New Way to Read a CBC
Most physicians glance at the CBC only to identify infection or anemia. But hidden within the differential may be powerful signals about long-term disease risk.
An elevated MLR should encourage broader evaluation, may include some of the following:
hs-CRP
Fasting insulin
Homocysteine
ApoB
Hemoglobin A1c
Uric acid (ideal target below 5.5 mg/dL)
Vitamin D
Omega-3 index
Ferritin
Uric Acid
The future of medicine increasingly lies in detecting dysfunction long before disease becomes clinically obvious.
Related Topics
You may also enjoy:
Bottom Line
A simple complete blood count may reveal far more than most physicians realize. The monocyte-to-lymphocyte ratio is emerging as a valuable marker of chronic inflammation, vascular injury, immune dysfunction, and potentially future dementia risk.The most important lesson is clear:
Cognitive decline does not begin when memory loss begins. It often starts decades earlier through inflammatory and metabolic pathways that modern testing can increasingly detect.
By identifying these subtle warning signs early, patients may have an opportunity to intervene while preserving brain health for decades to come.
Become a Patient
At Stages of Life Medical Institute, we focus on identifying hidden drivers of accelerated aging before disease becomes irreversible.
Through advanced metabolic testing, inflammatory biomarker analysis, cognitive screening, hormone evaluation, and personalized longevity medicine, we help patients proactively protect long-term health.
To learn more, visit Stages of Life Medical Institute.
References
¹ Holmes C et al. Systemic inflammation and progression of Alzheimer disease. Neurology. 2009. PubMed: https://pubmed.ncbi.nlm.nih.gov/19139364/
² Perry VH et al. Systemic infections and inflammation affect chronic neurodegeneration. Nat Rev Immunol. 2007.PubMed: https://pubmed.ncbi.nlm.nih.gov/17676034/
³ Heneka MT et al. Neuroinflammation in Alzheimer disease. Lancet Neurol. 2015. PubMed: https://pubmed.ncbi.nlm.nih.gov/25792098/
⁴ Cunningham C et al. Microglial activation and neurodegeneration. Brain. 2005. PubMed: https://pubmed.ncbi.nlm.nih.gov/15689386/
⁵ Frasca D et al. Inflammaging and immune aging. Nat Rev Immunol. 2018. PubMed: https://pubmed.ncbi.nlm.nih.gov/29449638/
⁶ Bettcher BM et al. Peripheral inflammation and cognition. J Neuroinflammation. 2012. PubMed: https://pubmed.ncbi.nlm.nih.gov/22272745/
⁷ Kinney JW et al. Inflammation as central mechanism in Alzheimer disease. Alzheimers Dement. 2018. PubMed: https://pubmed.ncbi.nlm.nih.gov/29699843/
⁸ Heppner FL et al. Immune attack in Alzheimer disease. Nat Rev Neurosci. 2015. PubMed: https://pubmed.ncbi.nlm.nih.gov/25503976/
⁹ Calsolaro V et al. Neuroinflammation in Alzheimer disease. Mediators Inflamm. 2016. PubMed: https://pubmed.ncbi.nlm.nih.gov/27445440/
¹⁰ De Strooper B et al. Future directions in Alzheimer disease prevention. Cell. 2016. PubMed: https://pubmed.ncbi.nlm.nih.gov/27984715/
The medical references cited in this article are provided for educational purposes only and are intended to support general scientific discussion. They are not a substitute for individualized medical advice, diagnosis, or treatment. Clinical decisions should always be made in consultation with a qualified healthcare professional who can account for a patient’s unique medical history, medications, and circumstances.


1917 Boothe Circle, Suite 171
Longwood, Florida 32750
Tel: 407-679-3337
Fax: 407-678-7246



.webp)