

Avoid Vitamin D2, use Vitamin D3
- David S. Klein, MD FACA FACPM

- Apr 22
- 4 min read
And Why Vitamin D₃ Is Almost Always Preferred in Clinical Practice
Many patients are surprised to learn that not all vitamin D supplements are the same. Labels may simply say “vitamin D,” but there are two very different forms commonly used: vitamin D₂ (ergocalciferol) and vitamin D₃ (cholecalciferol).
From a physician’s standpoint, this distinction matters. Vitamin D₃ is almost always the superior choice for correcting deficiency and supporting long-term health.¹⁻³

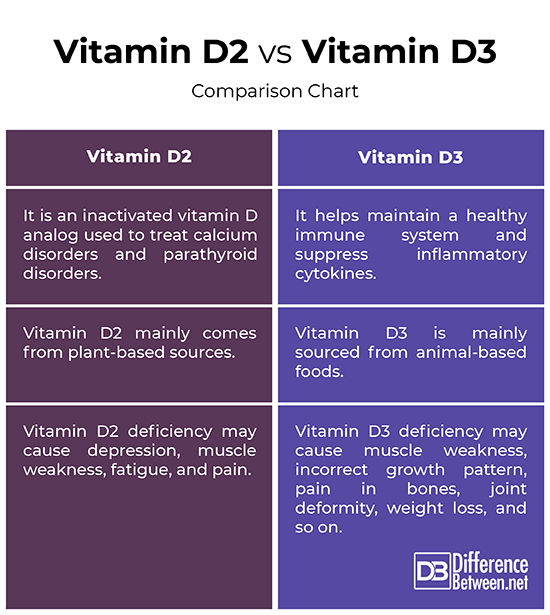
Vitamin D₂ vs Vitamin D₃: A Brief Overview
Vitamin D exists in two major supplemental forms:
Vitamin D₂ (ergocalciferol) – derived from plant sources and fungi
Vitamin D₃ (cholecalciferol) – biologically identical to the form synthesized in human skin following UVB exposure¹⁻³
Although both forms can raise vitamin D levels on laboratory testing, they are not biologically equivalent.²⁻⁶
The Biological Reality: D₂ and D₃ Are Not Interchangeable
After ingestion, both vitamin D₂ and D₃ undergo hepatic and renal hydroxylation to become hormonally active. However, substantial differences exist in their pharmacokinetics and biologic behavior.
Compared with vitamin D₂, vitamin D₃:
Raises serum 25-hydroxyvitamin D more efficiently²⁻⁷
Has a longer circulating half-life⁶⁻⁹
Binds more tightly to vitamin D–binding protein¹⁰
Produces fewer inactive metabolites⁴⁻⁶
These differences translate into more predictable and durable clinical responses with vitamin D₃.³⁻⁷
A Critical and Often Overlooked Issue: Vitamin D₂ Can Suppress Vitamin D₃
Beyond being less effective, vitamin D₂ introduces an additional problem rarely discussed in patient-facing literature: it can actively reduce circulating vitamin D₃ levels.
Controlled studies demonstrate that supplementation with vitamin D₂ increases serum 25-hydroxyvitamin D₂ while simultaneously decreasing endogenous 25-hydroxyvitamin D₃.²⁻³
This competitive effect is believed to result from shared hepatic hydroxylation pathways and weaker binding of D₂ metabolites to vitamin D–binding protein, leading to accelerated clearance of vitamin D₃, the body’s preferred and more biologically active form.²,³,¹⁰
Clinically, this means vitamin D₂ may paradoxically blunt overall vitamin D hormonal effectiveness, particularly in patients who require stable levels for bone, immune, neuromuscular, or cognitive health.²⁻⁴
Stability and Potency: Why D₂ Falls Short
Vitamin D₂ is chemically less stable than vitamin D₃, which affects shelf stability, serum persistence, and dosing reliability.⁴⁻⁶
In contrast, vitamin D₃ produces:
Higher peak serum 25-hydroxyvitamin D levels⁶⁻⁸
More sustained concentrations over time⁶⁻⁹
Greater consistency across repeated dosing⁷⁻⁹
These properties make vitamin D₃ far easier to monitor and titrate in clinical practice.
What Physicians Observe in Practice
Patients using vitamin D₂ frequently demonstrate:
Smaller increases in serum 25-hydroxyvitamin D²⁻⁶
Faster declines after supplementation stops⁶⁻⁹
Greater inter-patient variability⁷⁻⁹
Vitamin D₃, by contrast, shows reliable repletion, predictable dose-response relationships, and superior long-term stability.³⁻⁹
Clinical Outcomes Favor Vitamin D₃
When clinically meaningful endpoints are examined—rather than short-term lab changes—vitamin D₃ consistently outperforms vitamin D₂.
Vitamin D₃ has demonstrated superior effects on:
Bone mineral density and fracture prevention¹¹⁻¹³
Parathyroid hormone suppression¹,¹¹
Muscle strength and fall reduction¹¹,¹⁴
Overall mortality risk in observational studies¹⁴
Vitamin D₂ has not shown equivalent consistency across these outcomes.⁴⁻⁶
Why Vitamin D₂ Is Still Used
Vitamin D₂ remains in use largely for historical and regulatory reasons:
Earlier pharmaceutical formulations favored ergocalciferol
It was easier to synthesize commercially decades ago
Some prescription products still contain high-dose D₂ and doctors often 'disgorge bad habits, slowly.'

However, availability does not imply equivalence, and modern evidence overwhelmingly favors vitamin D₃.³⁻⁷
Safety, Dosing, and Monitoring
Both forms are fat-soluble and require clinical oversight at higher doses. However, because vitamin D₃ mirrors endogenous hormone physiology, its dose-response behavior is better understood and more predictable.¹,³,¹²
This allows for safer targeting of optimal blood levels while minimizing toxicity risk.¹,¹²
The Takeaway
Although vitamin D₂ and vitamin D₃ share a name, they are not interchangeable therapies.
From a physician’s perspective:
Vitamin D₃ is more potent
More stable
Longer lasting
More physiologically appropriate
Most importantly, vitamin D₂ may interfere with vitamin D₃ itself, undermining effective hormonal signaling.²⁻⁴ For patients seeking durable improvements in bone health, immune resilience, muscle performance, and long-term disease prevention, vitamin D₃ is almost always the correct clinical choice.
References
Holick MF. Vitamin D deficiency. N Engl J Med. 2007.https://pubmed.ncbi.nlm.nih.gov/17634462/
Armas LAG, Hollis BW, Heaney RP. Vitamin D₂ is much less effective than vitamin D₃ in humans. J Clin Endocrinol Metab. 2004.https://pubmed.ncbi.nlm.nih.gov/15240628/
Tripkovic L, et al. Comparison of vitamin D₂ and vitamin D₃ supplementation. Am J Clin Nutr. 2012.https://pubmed.ncbi.nlm.nih.gov/22552031/
Houghton LA, Vieth R. The case against ergocalciferol (vitamin D₂). Am J Clin Nutr. 2006.https://pubmed.ncbi.nlm.nih.gov/16632698/
Heaney RP, et al. Vitamin D₃ is more potent than vitamin D₂. J Clin Endocrinol Metab. 2011.https://pubmed.ncbi.nlm.nih.gov/21177785/
Trang HM, et al. Evidence that vitamin D₃ increases serum 25(OH)D more efficiently. Am J Clin Nutr. 1998.https://pubmed.ncbi.nlm.nih.gov/9701188/
Lehmann U, et al. Bioavailability of vitamin D₂ and D₃. Am J Clin Nutr. 2013.https://pubmed.ncbi.nlm.nih.gov/23616527/
Logan VF, et al. Long-term vitamin D₃ supplementation vs D₂. Br J Nutr. 2013.https://pubmed.ncbi.nlm.nih.gov/23298705/
Jones KS, et al. Ergocalciferol vs cholecalciferol pharmacokinetics. Am J Clin Nutr. 2014.https://pubmed.ncbi.nlm.nih.gov/24695890/
Bouillon R, et al. Vitamin D binding protein and metabolism. Endocr Rev. 2019.https://pubmed.ncbi.nlm.nih.gov/30615155/
Bischoff-Ferrari HA, et al. Effect of vitamin D on falls. JAMA. 2004.https://pubmed.ncbi.nlm.nih.gov/15113819/
Rosen CJ, et al. Nonskeletal effects of vitamin D. Endocr Rev. 2012.https://pubmed.ncbi.nlm.nih.gov/22596255/
Pilz S, et al. Vitamin D and mortality risk. Am J Clin Nutr. 2009.https://pubmed.ncbi.nlm.nih.gov/19116333/
Annweiler C, et al. Vitamin D and cognition. J Intern Med. 2013.https://pubmed.ncbi.nlm.nih.gov/23489360/
Bikle DD. Vitamin D metabolism and clinical implications. Chem Biol. 2014.https://pubmed.ncbi.nlm.nih.gov/24529992/


1917 Boothe Circle, Suite 171
Longwood, Florida 32750
Tel: 407-679-3337
Fax: 407-678-7246




.webp)