

Sepsis and the Urinary Tract: Why Diagnosis Fails—And How We Fix It
- David Stephen Klein, MD FACA FACPM

- Apr 29
- 5 min read
A Clinical Perspective on Geriatric UTI, Dipstick Limitations, and PCR-Based Detection

Introduction
Sepsis remains one of the most consequential—and frequently misrecognized—conditions in clinical medicine. It is not merely infection; it is a failure of physiologic regulation in response to infection, resulting in organ dysfunction and, if untreated, death.¹
Among all infectious sources, the urinary tract is one of the most common origins of sepsis, particularly in older adults. Yet paradoxically, it is also one of the most poorly diagnosed, especially in nursing homes and outpatient geriatric care.²
The central issue is not a lack of testing—it is reliance on inadequate testing methods.
What Sepsis Is (Clinically Speaking)
Sepsis is best understood as:
Infection + organ dysfunction
The modern definition (Sepsis-3) describes sepsis as a dysregulated host response to infection leading to life-threatening organ dysfunction.¹
Once infection begins to impair cognition, renal function, respiration, circulation, or metabolic stability, the patient has crossed into sepsis.
In older adults, this transition is often subtle, rapid, and easily missed.
Clinical Significance
Sepsis is both common and dangerous:
Leading cause of hospitalization and mortality
Disproportionately affects adults over age 65
Frequently underrecognized early
Outcomes strongly tied to speed of diagnosis and treatment³
Early recognition is not simply beneficial—it is determinative.
Why the Urinary Tract Matters
Urinary infections are:
Common in both community and institutional settings
A frequent source of bacteremia and sepsis
Often misdiagnosed in both directions
This creates a dual clinical failure:
Overdiagnosis → unnecessary antibiotics
Underdiagnosis → progression to sepsis
Geriatric UTI: The Diagnostic Paradox
Older adults, particularly in nursing homes, present unique challenges:
High prevalence of asymptomatic bacteriuria
Atypical presentations (confusion, weakness, falls)
Reduced reporting of urinary symptoms
Importantly:
Bacteriuria alone does not equal infection⁴
Treating colonization exposes patients to harm without benefit.
The Nursing Home Problem
In long-term care settings, a familiar pattern emerges:
Patient develops confusion or decline
Urine is tested
Bacteria are found
Antibiotics are prescribed
This sequence is frequently incorrect.
Cloudy urine, odor, or a positive dipstick are not sufficient criteria for diagnosing UTI.⁵
At the same time, true infection may be missed when symptoms are subtle.
Where Traditional Testing Fails
Urine Dipstick Limitations
Dipsticks evaluate:
Nitrites
Leukocyte esterase
They are screening—not diagnostic—tools.
False negatives occur due to:
Non–nitrite-producing organisms
Frequent voiding
Vitamin C interference
Early infection
Dilute urine⁶
False positives occur due to:
Chronic inflammation
Colonization
Noninfectious causes of pyuria
A negative dipstick does not exclude infection. A positive dipstick does not confirm infection.
(See Figure 1: Limitations of Urine Dipstick Testing)

The Diagnostic Gap in UTI and Urosepsis
Traditional urine culture:
Requires 24–72 hours
Depends on organism growth conditions
May miss polymicrobial or fastidious organisms
This creates a dangerous clinical window where:
The patient deteriorates
Diagnosis remains uncertain
Treatment may be delayed or inappropriate
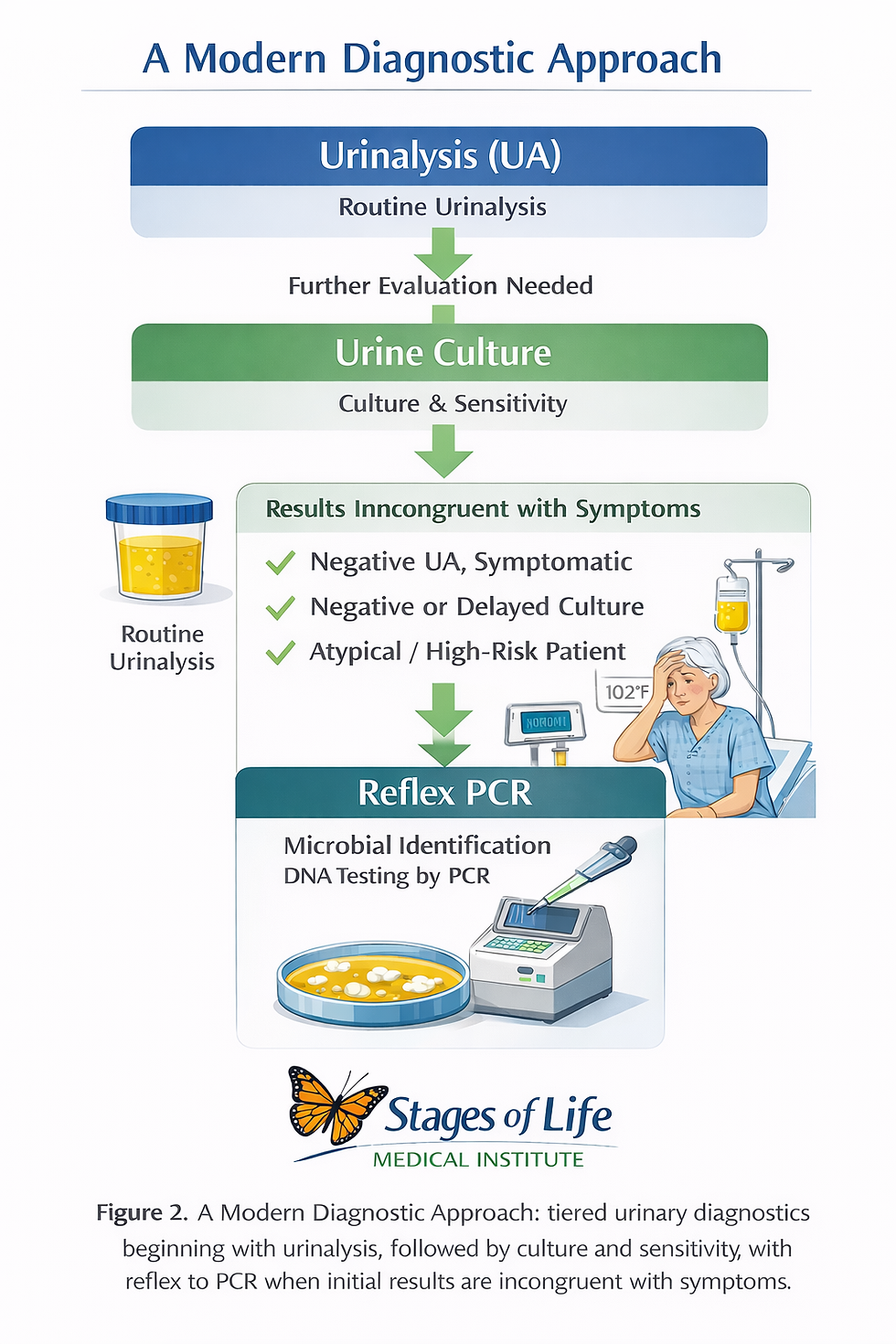
A Modern Diagnostic Strategy: UA → Culture → Reflex PCR
A practical and clinically sound approach is to begin with a routine urinalysis (UA) followed by culture and sensitivity (C&S), using these as the initial screening and organism-directed framework, and then reflexing to PCR-based testing when results are incongruent with the clinical picture.
UA provides rapid insight into inflammatory activity (pyuria, hematuria, nitrites), while culture allows for organism identification and antibiotic susceptibility—still essential for targeted therapy. However, both are limited by sensitivity, growth requirements, and time delay.
When a patient remains symptomatic despite a negative U, when cultures are repeatedly negative or slow-growing, or when the presentation is atypical—as is common in geriatric populations—PCR serves as a valuable second-line diagnostic tool, detecting microbial DNA independent of growth conditions and improving identification of polymicrobial or fastidious organisms.⁶–⁸
In this tiered model, UA and culture establish a cost-effective, standardized baseline, while PCR is deployed selectively to resolve diagnostic uncertainty and reduce both missed infections and inappropriate treatment.⁶–⁹
(See Figure 2: Diagnostic Pathway—Traditional vs PCR-Augmented Approach)
UTI Progression to Sepsis
In older adults, progression may be subtle:
Mild or absent urinary symptoms
Functional decline
Confusion or delirium
Dehydration
Renal dysfunction
Hypotension
Sepsis
Early diagnostic ambiguity is common—and dangerous.
(See Figure 3: Clinical Progression from UTI to Urosepsis)

Clinical Decision Framework
Step 1: Assess for symptoms
Dysuria, urgency, frequency
Fever, flank pain
Hemodynamic instability
Step 2: Recognize atypical presentations
Confusion
Weakness
Functional decline
Evaluate for systemic illness.
Step 3: Apply appropriate testing
Clinical Scenario | Recommended Approach |
Classic UTI | UA + culture |
Atypical geriatric | UA + culture ± PCR |
Recurrent or refractory | PCR strongly indicated |
Suspected sepsis | Full evaluation + targeted diagnostics |
Prognosis
Outcomes depend on:
Speed of recognition
Accuracy of diagnosis
Timeliness of treatment
Older adults face:
Higher mortality
Increased functional decline
Greater recurrence risk³
However, early and accurate diagnosis significantly improves outcomes.
Bottom Line
Sepsis is a medical emergency defined by infection causing organ dysfunction.
In older adults, urinary infections are a common pathway—but diagnosis is complicated by:
Asymptomatic bacteriuria
Atypical presentation
Dipstick limitations
Delayed or incomplete culture data
A negative dipstick does not rule out infection. A positive dipstick does not confirm it.
A modern, tiered diagnostic approach—UA followed by culture, with reflex to PCR when needed—offers a more accurate, clinically effective strategy.
Call to Action
If you or a loved one is experiencing:
Recurrent urinary symptoms
Confusion without clear explanation
Persistent symptoms despite negative testing
Concern for early infection or sepsis
A more advanced diagnostic approach may be warranted.
At Stages of Life Medical Institute, we integrate traditional clinical evaluation with advanced diagnostic tools—including PCR-based testing—to improve accuracy and patient outcomes.
👉 Become a Patient: https://stagesoflifemedicalinstitute.com
References
Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):801–810.
https://pubmed.ncbi.nlm.nih.gov/26903338/
Hooton TM. Clinical practice. Uncomplicated urinary tract infection. N Engl J Med. 2012;366(11):1028–1037. https://pubmed.ncbi.nlm.nih.gov/22417256/
Rhee C, Dantes R, Epstein L, et al. Incidence and trends of sepsis in US hospitals. JAMA. 2017;318(13):1241–1249. https://pubmed.ncbi.nlm.nih.gov/28903154/
Nicolle LE, Gupta K, Bradley SF, et al. Clinical practice guideline for asymptomatic bacteriuria. Clin Infect Dis. 2019;68(10):e83–e110.
https://pubmed.ncbi.nlm.nih.gov/30895288/
Loeb M, Bentley DW, Bradley S, et al. Development of minimum criteria for antibiotics in long-term care. Infect Control Hosp Epidemiol. 2001;22(2):120–124.
Simerville JA, Maxted WC, Pahira JJ. Urinalysis: A comprehensive review. Am Fam Physician. 2005;71(6):1153–1162.
Price TK, Dune T, Hilt EE, et al. Enhanced urine culture techniques. J Clin Microbiol. 2016;54(5):1216–1222. https://pubmed.ncbi.nlm.nih.gov/26962083/
Khasriya R, Sathiananthamoorthy S, Ismail S, et al. Bacterial colonization in LUTS. J Clin Microbiol. 2013;51(7):2054–2062. https://pubmed.ncbi.nlm.nih.gov/23637317/
Wolfe AJ, Brubaker L. “Sterile urine” reconsidered. Clin Microbiol Rev. 2015;28(3):719–733. https://pubmed.ncbi.nlm.nih.gov/25985967/
The medical references cited in this article are provided for educational purposes only and are intended to support general scientific discussion. They are not a substitute for individualized medical advice, diagnosis, or treatment. Clinical decisions should always be made in consultation with a qualified healthcare professional who can account for a patient’s unique medical history, medications, and circumstances.


1917 Boothe Circle, Suite 171
Longwood, Florida 32750
Tel: 407-679-3337
Fax: 407-678-7246



.webp)