

Pre-Diabetes: Insulin Resistance, Is It a Real Condition — Or a Warning Sign We Ignore at Our Own Risk?
- David Stephen Klein, MD FACA FACPM

- Jul 3
- 6 min read

Quick Look
Many people are told they have pre-diabetes and assume it simply means they may someday develop diabetes. The truth is far more concerning. Long before someone officially develops Type 2 diabetes, elevated insulin levels and subtle abnormalities in blood sugar regulation may already be damaging blood vessels, nerves, kidneys, and even the brain.¹²
Prediabetes is not almost disease.
It is often the earliest measurable sign that metabolic dysfunction has already begun.
The good news is that early intervention can frequently reverse the process entirely.
Pre-Diabetes Is Not a Harmless Laboratory Finding
One of the most dangerous misunderstandings in medicine is the idea that pre-diabetes is not a real disease. Patients commonly hear:
“Your sugar is a little high… but you’re not diabetic yet.”
Unfortunately, this statement often creates a false sense of security. Prediabetes represents metabolic dysfunction that may have been silently developing for ten years or longer before formal diabetes is ever diagnosed.¹
By the time glucose levels consistently rise, substantial injury may already be underway.
What Exactly are Insulin Resistance and Pre-Diabetes?
Prediabetes is generally defined as one or more of the following:
Hemoglobin A1c: 5.6% – 6.4%
Fasting blood glucose: 100–125 mg/dL
Abnormal oral glucose tolerance testing
Normal physiology depends on insulin moving glucose from the bloodstream into cells where it is used for energy.
In pre-diabetes, cells begin responding poorly to insulin.
This condition is called insulin resistance.²³
The pancreas compensates by producing progressively larger amounts of insulin in an attempt to keep blood sugar controlled.
In our practice, we begin paying very close attention once hemoglobin A1c rises above 5.5%, as meaningful metabolic dysfunction may already be developing well before conventional diabetic thresholds are reached.⁵⁶
The Real Problem Often Starts With Insulin
Many people believe glucose is the primary problem.
In reality, elevated glucose is often a late finding.
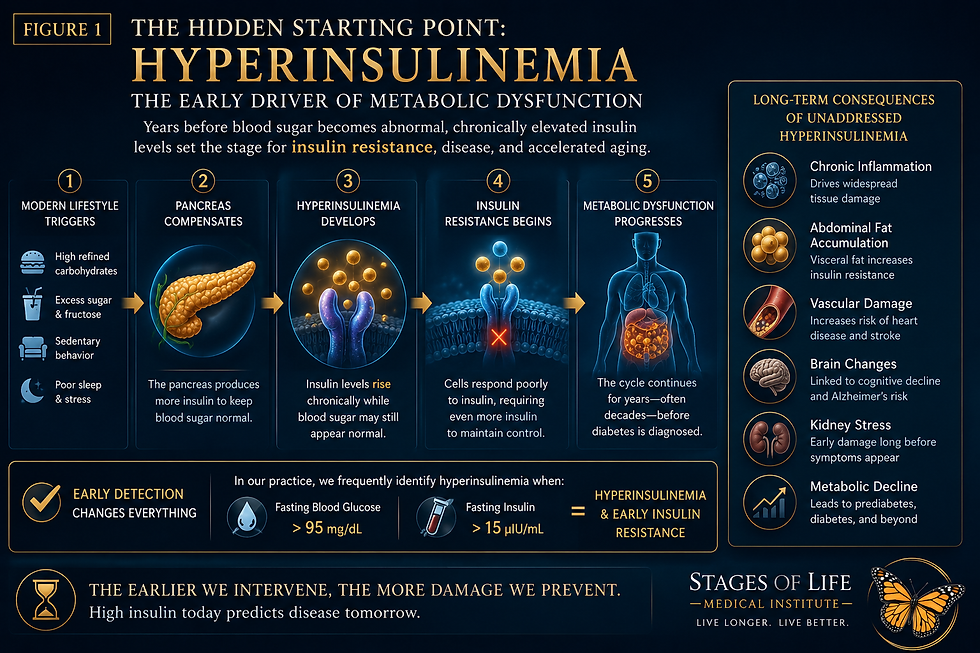
The earliest abnormality frequently begins with hyperinsulinemia — chronically elevated insulin levels in the bloodstream long before diabetes develops.²⁸
Hyperinsulinemia develops when the body’s cells become progressively resistant to insulin signaling.
In response, the pancreas compensates by producing increasingly larger amounts of insulin in an effort to keep blood sugar controlled. This process may continue silently for years while glucose values remain within what conventional medicine considers a “normal range.”
Excess insulin contributes to:
In our practice, we frequently identify hyperinsulinemia when fasting blood glucose rises above approximately 95 mg/dL while fasting insulin exceeds 15 µIU/mL.
At this stage, a patient may not yet meet conventional criteria for diabetes or even prediabetes — but important metabolic dysfunction is already underway.
This process may quietly progress for years before diabetes is formally diagnosed.
Prediabetes and Life Expectancy
One of the more concerning observations emerging from metabolic medicine is that measurable health consequences begin appearing well before a patient becomes diabetic.
Large population studies demonstrate that life expectancy begins to progressively decline once hemoglobin A1c rises above approximately 5.5%, even when values remain below the conventional threshold used to diagnose diabetes.⁶
The body does not wait until diabetes develops before metabolic injury begins. As blood sugar gradually rises, cumulative inflammation, oxidative stress, endothelial dysfunction, vascular injury, and insulin resistance begin accelerating biological aging itself.In practical terms, every incremental rise in hemoglobin A1c above the optimal range may represent gradual shortening of health span and potentially life expectancy. Waiting until a patient officially “becomes diabetic” often means waiting until years of silent metabolic injury have already occurred.
Clinical Pearl
One of the greatest limitations of conventional metabolic screening is that fasting glucose alone frequently misses early metabolic disease. A patient may present with a fasting glucose that appears normal while insulin levels have already been elevated for years.
At our clinic, we pay close attention when:
Fasting blood glucose exceeds 95 mg/dL
Fasting insulin exceeds 15 µIU/mL
This combination frequently indicates hyperinsulinemia and early insulin resistance, even when hemoglobin A1c has not yet reached formal prediabetic range.
Useful early markers often include:
Fasting insulin
Triglyceride to HDL ratio
Waist circumference
High sensitivity CRP
Post meal glucose monitoring
Continuous glucose monitoring
Waiting until glucose becomes clearly abnormal often means metabolic injury has already been progressing for years. The earliest detectable disease frequently begins not with high sugar — but with high insulin.²⁸
Prediabetes and Cardiovascular Disease
Elevated blood sugar causes cumulative injury to blood vessels.
Imagine compressed air sprayed against a painted wall.
Air alone causes no damage.
But add fine sand particles, and over time the paint erodes.
Continue long enough and eventually the wall itself becomes damaged.
Glucose behaves similarly. Even modest elevations gradually injure the delicate endothelial lining inside blood vessels.
This increases risk for:
Coronary artery disease
Stroke
Peripheral vascular disease
Kidney disease
Progressive hypertension⁵

The Brain Is Affected Long Before Diabetes Develops
Emerging research increasingly links insulin resistance to neurodegenerative disease.
Some researchers now refer to Alzheimer's Disease as Type 3 Diabetes.⁷
Insulin resistance contributes to:
Neuroinflammation
Reduced glucose utilization within neurons
Increased beta amyloid deposition
Increased tau protein accumulation
Accelerated cognitive decline
Long before diabetes develops, the brain may already be experiencing metabolic stress.
Can Pre-Diabetes Be Reversed?
The answer is often yes. And the earlier intervention begins, the better the outcome.⁹¹⁰
Nutrition
Eliminate processed carbohydrates
Reduce sugar intake
Limit excess fructose consumption
Increase dietary fiber
Prioritize adequate protein intake
Exercise
Resistance training
Walking after meals
Building lean muscle mass
Sleep
Optimize sleep quality
Evaluate for sleep apnea
Support circadian rhythm
Weight Reduction
Even 5–7% weight reduction frequently improves metabolic health.
Advanced Testing
Fasting insulin
Continuous glucose monitoring
Advanced metabolic testing
Body composition analysis
Bottom Line
Pre-diabetes is absolutely real. It represents the earliest measurable phase of metabolic dysfunction that may eventually progress toward diabetes, cardiovascular disease, dementia, obesity, and accelerated aging. Unlike many chronic illnesses, this process is often reversible.
The key is recognizing warning signs early enough to intervene before permanent damage occurs. Health decline does not begin the day diabetes is diagnosed. It usually begins years earlier.
Related Topics
• Insulin Resistance: The Hidden Driver of Chronic Disease
• Metabolic Syndrome Explained
• Why Magnesium Deficiency Worsens Blood Sugar Contro
l• Berberine and Natural Blood Sugar Support
• Why Poor Sleep Increases Weight Gain and Insulin Resistance
Become a Patient
At Stages of Life Medical Institute, we focus on identifying metabolic dysfunction before disease becomes irreversible. Advanced metabolic testing frequently reveals problems years before traditional screening methods detect them. Early diagnosis changes outcomes.
The future of your health is being built today.
References
¹ Tabák AG, et al. Prediabetes: a high-risk state for diabetes development. Lancet. 2012.PMID: 22683128PubMed Abstract
² Reaven GM. Role of insulin resistance in human disease. Diabetes. 1988.PMID: 3056758PubMed Abstract
³ DeFronzo RA. Pathogenesis of type 2 diabetes mellitus. Med Clin North Am. 2004.PMID: 15308380PubMed Abstract
⁴ American Diabetes Association. Standards of Care in Diabetes 2026.ADA Standards of Care
⁵ Huang Y, et al. Prediabetes and cardiovascular disease risk. BMJ. 2016.PMID: 27815263PubMed Abstract
⁶ Khaw KT, et al. Hemoglobin A1c and mortality. BMJ. 2001.PMID: 11141143PubMed Abstract
⁷ Craft S. Insulin resistance and Alzheimer disease pathogenesis. Lancet Neurol. 2012.PMID: 23079501PubMed Abstract
⁸ Petersen MC, Shulman GI. Mechanisms of insulin resistance. Physiol Rev. 2018.PMID: 30067154PubMed Abstract
⁹ Knowler WC, et al. Diabetes Prevention Program. NEJM. 2002.PMID: 11832527PubMed Abstract
¹⁰ Taylor R. Reversal of Type 2 Diabetes. Diabetologia. 2019.PMID: 31236777PubMed Abstract
The medical references cited in this article are provided for educational purposes only and are intended to support general scientific discussion. They are not a substitute for individualized medical advice, diagnosis, or treatment. Clinical decisions should always be made in consultation with a qualified healthcare professional who can account for a patient’s unique medical history, medications, and circumstances.


1917 Boothe Circle, Suite 171
Longwood, Florida 32750
Tel: 407-679-3337
Fax: 407-678-7246




.webp)