

Levator Scapulae Syndrome: The Culprit of Neck Pain
- David S. Klein, MD FACA FACPM
- May 11
- 8 min read
Levator scapulae syndrome is one of the most underdiagnosed causes of chronic neck and shoulder pain. A 2026 review in Frontiers in Public Health found that 55-69% of computer users now report neck pain, and clinical research shows up to 93% of office workers with neck and scapular complaints have measurable tightness in the levator scapulae muscle. Patients describe a deep ache at the base of the neck, pain that travels into the shoulder blade, and a tight "rope" running from the skull down to the shoulder. The good news: when correctly identified, levator scapulae syndrome is one of the more treatable musculoskeletal pain conditions. This guide covers what the levator scapulae actually does, why it gets injured, the symptoms to watch for, and the stretches and treatments that work — based on what we see every week at Stages of Life Medical Institute in Longwood, Florida.
Understanding the Anatomy

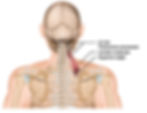
The levator scapulae is a slender, strap-like muscle on the side and back of the neck. It originates from the transverse processes of the first four cervical vertebrae (C1-C4) and inserts on the upper inner border of the scapula. Its job, as the name suggests, is to elevate the shoulder blade — every time you shrug, look down at your phone, or carry a heavy bag, your levator scapulae fires. Because it spans the neck and shoulder simultaneously, it is uniquely vulnerable to overuse. A 2022 study in the International Journal of Occupational Safety and Ergonomics found that 90% of office workers with neck and scapular pain show measurable scapular dyskinesis — abnormal scapular movement that overloads the levator scapulae. The brachial plexus, the nerve bundle that supplies the arm, runs in close proximity, which is why levator scapulae problems can radiate pain or tingling into the shoulder, upper back, and even the fingers.
Understanding why the levator scapulae becomes injured is the first step toward effective treatment. In our clinic, most cases trace back to a small number of common triggers that build up over weeks or months of repetitive strain.

What Causes Levator Scapulae Syndrome?
Nerve entrapment at the levator scapulae can result from several factors, including:
Forward Head Posture and Desk Work: Roughly 43% of office workers with neck pain show measurable forward head posture, and 100% show rounded shoulders (Tandfonline, 2022). Every inch the head shifts forward roughly doubles the load on the posterior neck muscles — the levator scapulae carries that load.
Repetitive and Asymmetric Strain: Carrying a bag on the same shoulder, painting ceilings, sleeping on your stomach with the head turned, holding a phone between ear and shoulder, or working at a tilted or off-axis monitor all chronically shorten the levator scapulae. The body adapts to whatever position it spends the most time in, and the levator scapulae rarely wins that battle.
Stress and Bracing: Mental stress drives unconscious shoulder elevation, and the levator scapulae is one of the first muscles to grip when we tense up. Over weeks of repetitive bracing, that elevated resting tone becomes the new baseline and the muscle stays tight even at rest. We see the strongest correlation in patients with high-demand jobs, poor sleep, or unresolved anxiety.
Cervical or Shoulder Injury: Whiplash, slip-and-fall accidents, lifting injuries, and rotator-cuff problems all disturb scapular mechanics and overload the levator scapulae. Roughly half of whiplash patients still report neck pain months after the original event, frequently centered on the levator attachment at the upper inner border of the shoulder blade.
Degenerative Cervical Changes: Arthritic changes at the C4-C5 and C5-C6 segments are common with age and can refer pain into the levator scapulae and trigger compensatory tightness around the muscle. We see this pattern most often in patients over 50, especially those with a history of prolonged desk work or repetitive overhead labor.
Understanding these triggers is the first step toward effective treatment. The good news is that for most patients, levator scapulae syndrome responds well to conservative care — stretching, postural correction, and targeted manual therapy. Surgery is almost never indicated.

Symptoms to Watch For
Identifying the symptoms of nerve entrapment in the levator scapulae area is essential for timely intervention. Common symptoms include:
Localized Pain: Sharp or dull pain localizing in the neck and upper shoulder region.
Radiating Pain: Discomfort that travels down the arm, potentially into the shoulder.
Numbness or Tingling: A tingling sensation in the arm or hand, indicating nerve compression.
Muscle Weakness: Difficulty raising the arm or gripping objects due to muscle weakness linked to nerve irritation.
If symptoms persist beyond 2 weeks, radiate down the arm, or include numbness, tingling, or weakness, see a clinician. Persistent radicular symptoms can indicate cervical nerve root involvement and warrant imaging. Patients in the Orlando and Longwood area can request an evaluation through our Pain Management program at Stages of Life Medical Institute.

Diagnosis and Treatment Options
To diagnose nerve entrapment, healthcare providers will conduct a comprehensive medical history and physical examination. Techniques such as MRI or ultrasound may be employed to evaluate the structures near the levator scapulae.
Once diagnosed, effective treatment options include:
Physical Therapy: A skilled physical therapist combines soft-tissue release, scapular stabilization (lower-trapezius and serratus-anterior strengthening), and motor re-education. A 2024 Cochrane review of conservative care for chronic neck pain found supervised exercise therapy reduces pain scores by 30 to 50% versus usual care, with effects holding at 12-month follow-up.
Chiropractic Care: Targeted cervical and upper-thoracic adjustments can restore segmental motion and reduce the compensatory load on the levator scapulae. We see the best outcomes when chiropractic is paired with active rehab, not used as a standalone fix. Refer-in to a chiropractor with neuromusculoskeletal training rather than a pure-adjustment practice.
Massage Therapy: Therapeutic massage can reduce muscle tension and promote relaxation in the affected area. Research shows that around 70% of patients experience relief from chronic neck pain following regular massage.
Pain Management: Anti-inflammatory medications or corticosteroid injections may temporarily relieve pain and swelling. An estimated 30 to 90% of those suffering from neck pain find relief through these medications, and injections often provide immediate relief.
Home Care: Utilizing heat or cold packs, along with gentle stretching exercises at home, may assist in symptom management.
Topical Medications: Topical anti-inflammatories deliver medication straight to the levator scapulae insertion at the upper inner border of the scapula, producing concentrated relief without systemic side effects. The two we use and recommend daily in clinic are Kink-Ease MSM Salve (developed by Dr. Klein and stocked through our practice) and Voltaren (topical diclofenac, now available over the counter). Alternating the two through the day tends to outperform either alone.

Voltaren topical diclofenac is now OTC available. 
Kink-Ease MSM Cream 16 oz. $44.95/bottle Three for $114.62
Recognizing the appropriate interventions is key to alleviating pain and restoring function.
Preventative Measures
Preventing nerve entrapment requires attention to posture and lifestyle habits. Here are some strategies to consider:
Maintain Proper Posture: Ensure your sitting and standing positions support a neutral spine. Ergonomically designed office equipment can greatly enhance posture.
Incorporate Regular Exercise: Engage in activities that promote flexibility and strength in the neck and shoulders, reducing tension and future pain episodes.
Take Frequent Breaks: For those in desk jobs, taking regular breaks to stand, move around, and stretch can combat muscle tightness. A break every hour can significantly reduce discomfort.
Manage Stress: Use relaxation techniques such as yoga, meditation, or deep breathing exercises to lessen muscle tension and anxiety.
Implementing these preventative measures can significantly decrease the likelihood of encountering neck and shoulder pain in the future.
Levator Scapulae Stretches You Can Do at Home
These three stretches form the at-home protocol we recommend to patients. Do each one 2 to 3 times per day, hold each stretch for 30 seconds, and repeat both sides even if only one side hurts.
Classic Levator Scapulae Stretch: Sit tall. Drop your right ear toward your right armpit. Rotate your chin 45 degrees down toward your right armpit, as if smelling under your arm. Place your right hand on top of your head and apply gentle downward pressure. Reach the left arm down and press the fingertips toward the floor to anchor the left scapula. Hold 30 seconds. You should feel a long, ropey stretch from the base of the skull to the inner shoulder blade. Repeat on the other side.
Wall-Anchored Scapular Set: Stand with your back flat against a wall, heels 2 to 3 inches out. Press the back of your head, upper back, and tailbone into the wall. Slide your arms up the wall in a goalpost position, keeping the backs of the wrists touching the wall. Hold 5 seconds, lower, repeat 10 times. This trains the lower trapezius to take load off the levator scapulae.
Self-Massage with a Lacrosse Ball: Place a lacrosse ball or tennis ball between your upper inner shoulder blade and a wall. Slowly roll the ball over the tender area for 60 to 90 seconds. Avoid pressing directly on the spine. Mild discomfort is normal; sharp pain is not.
Frequently Asked Questions
How long does levator scapulae syndrome take to heal?
Most uncomplicated cases resolve in 2 to 6 weeks with consistent stretching, postural correction, and topical anti-inflammatories. Cases involving an underlying cervical issue or chronic ergonomic strain may take 8 to 12 weeks of structured rehabilitation.
What is the ICD-10 code for levator scapulae syndrome?
Levator scapulae syndrome typically codes under M25.819 (other specified disorder of unspecified joint, shoulder region) or M62.838 (other muscle spasm) depending on presentation. M54.2 (cervicalgia) is used when neck pain is the dominant symptom. Your clinician will choose the most accurate code based on exam findings.
Can levator scapulae syndrome cause headaches?
Yes, and this is one of the most missed diagnoses we see. The levator scapulae shares fascial and neural connections with the suboccipital muscles at the base of the skull. Chronic levator scapulae tension routinely refers into a tight band that wraps around the back of the head and behind the eyes, presenting as a tension-type headache.
Is heat or ice better for levator scapulae pain?
In the first 24 to 48 hours after a flare-up, ice for 15 minutes at a time helps reduce inflammation. After that, moist heat from a hot shower or a heated rice pack relaxes the muscle and is more therapeutic. The rule we tell patients: ice for swelling, heat for stiffness.
Taking Action on Your Health
Levator scapulae syndrome is one of the easier neck pain diagnoses to miss and one of the easier to fix once it is spotted. The pattern is recognizable: a tight rope from skull to shoulder blade, pain that worsens when you turn the head away from it, and a stiff neck most mornings. The protocol in this guide — postural correction, the three home stretches above, topical anti-inflammatories, and short courses of NSAIDs — resolves most cases in 2 to 6 weeks. If your pain has lasted longer than two weeks, radiates down the arm, or comes with numbness, tingling, or weakness, that is a clinic visit. We see and treat levator scapulae syndrome every week at Stages of Life Medical Institute in Longwood, Florida. Call 407-679-3337 or request a new patient appointment to be seen this week.
REFERENCES:
Henry C, Reidler J. Levator Scapulae Syndrome. StatPearls Publishing; 2024. https://www.ncbi.nlm.nih.gov/books/NBK556128/
Cohen SP, Hooten WM. Advances in the diagnosis and management of neck pain. BMJ. 2017;358:j3221. https://www.bmj.com/content/358/bmj.j3221
Khaledi A, et al. Investigation of postural abnormalities in office workers with neck pain. International Journal of Occupational Safety and Ergonomics. 2022;28(4). https://www.tandfonline.com/doi/full/10.1080/10803548.2021.1916206
Physiopedia. (n.d.). Levator scapulae syndrome. https://www.physio-pedia.com/Levator_Scapulae_Syndrome
OrthoFixar. (n.d.). Overview of levator scapulae pain causes and treatment. https://orthofixar.com/for-patient/levator-scapulae-pain-treatment
Release Muscle Therapy. (n.d.). Levator scapulae pain: Unraveling the mystery and finding relief. https://releasemuscletherapy.com/pain-in-levator-scapulae-relief
Leagrave Therapy. (n.d.). Neck pain and levator scapulae syndrome. https://www.leagravetherapy.co.uk/levator-scapulae-syndrome-and-neck-pain
Physiopedia. (n.d.). Levator scapulae. https://www.physio-pedia.com/Levator_Scapulae
Physio.co.uk. (n.d.). Levator scapulae syndrome. https://www.physio.co.uk/what-we-treat/musculoskeletal/conditions/shoulder/levator-scapulae-syndrome.php
Bel Marra Health. (n.d.). How is levator scapulae pain related to stiff neck and how to relieve the pain?. https://www.belmarrahealth.com/levator-scapulae-pain-causes-symptoms-treatment-exercises
Physical Therapy. (n.d.). Levator scapulae muscle pain: Cause, treatment, exercise. https://physical-therapy.us/levator-scapulae-muscle-pain
Physio Insights. (n.d.). Levator scapulae pain. https://physioinsights.com/2020/12/31/levator-scapulae-pain
NSMI. (n.d.). Levator scapulae syndrome - Muscular injuries. https://www.nsmi.org.uk/articles/muscular-injuries/levator-scapulae-syndrome.html


David S. Klein, MD, FACA, FACPM
1917 Boothe Circle, Suite 171
Longwood, Florida 32750
Tel: 407-679-3337
Fax: 407-678-7246

.webp)