

How Does Low Vitamin D Harm Kidney Function?
- David Stephen Klein, MD FACA FACPM

- Feb 11
- 5 min read
Vitamin D deficiency is often discussed in terms of bone health, immunity, or fatigue. Far less appreciated is its quiet but meaningful impact on kidney structure, filtration, and long-term renal resilience.
Vitamin D deficiency is often treated as a minor or incidental laboratory finding—something relevant to bone density, immune support, or seasonal fatigue. From a physiological and nephrologic standpoint, that framing is incomplete and, in many cases, misleading.
The kidneys are not passive targets of vitamin D status.
They are central endocrine organs responsible for converting vitamin D into its biologically active hormonal form. When vitamin D levels are chronically low, the kidneys are exposed to increased hormonal stress, inflammation, vascular injury, and fibrotic signaling—often years before traditional markers such as serum creatinine or estimated glomerular filtration rate (eGFR) reveal overt disease¹².
This article explains how low vitamin D harms kidney function, why this relationship is frequently overlooked, and how vitamin D deficiency can quietly accelerate renal decline.
Vitamin D Is a Kidney-Activated Hormone

Vitamin D is unique among nutrients. Rather than acting directly, it must undergo two enzymatic activation steps, the second of which occurs in the kidneys³.
The pathway includes:
Cutaneous synthesis or dietary intake of vitamin D₃ (cholecalciferol)
Hepatic conversion to 25-hydroxyvitamin D [25(OH)D]
Renal conversion to 1,25-dihydroxyvitamin D (calcitriol), the active hormone⁴
This final step occurs in the proximal renal tubules and is tightly regulated by parathyroid hormone (PTH), phosphate balance, fibroblast growth factor-23 (FGF-23), and inflammatory signaling⁵.
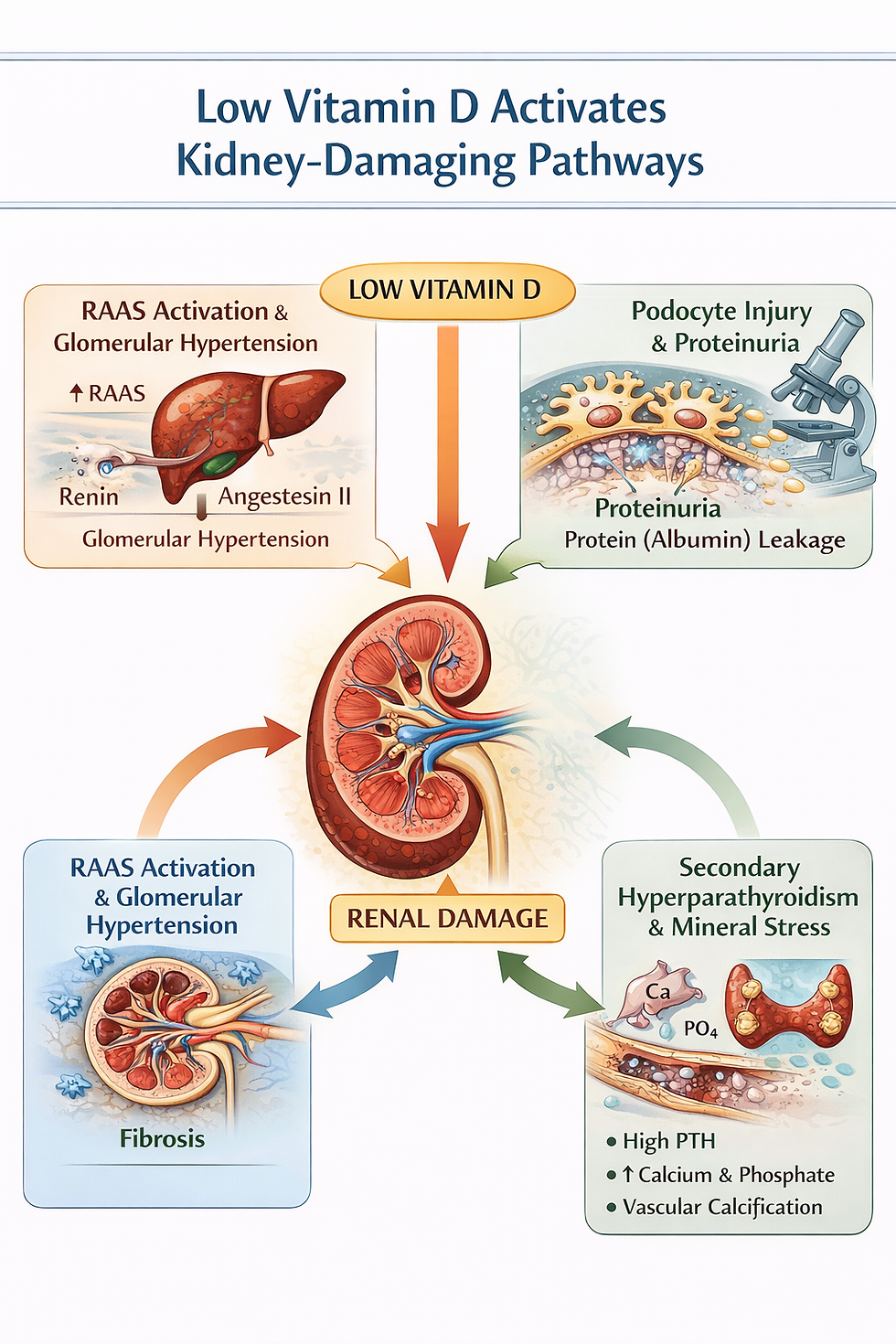
When vitamin D levels are low, this endocrine system becomes dysregulated, placing the kidneys in a maladaptive physiological state (see Figure 1).
Low Vitamin D Activates the Renin–Angiotensin–Aldosterone System
One of vitamin D’s most important renal functions is suppression of renin expression.
Experimental and clinical data demonstrate that active vitamin D:
Suppresses renin gene transcription
Reduces angiotensin II production
Limits intraglomerular hypertension⁶⁷
When vitamin D is deficient:
Renin activity increases
Angiotensin II rises
Efferent arteriolar constriction worsens
Glomerular pressure increases
This promotes glomerular hyperfiltration and structural injury, accelerating nephron loss and albuminuria⁸. Notably, these changes may occur before systemic hypertension becomes clinically apparent, allowing kidney damage to progress silently.
Vitamin D Deficiency Promotes Renal Fibrosis
Fibrosis represents the final common pathway of chronic kidney disease.
Vitamin D signaling normally inhibits fibrotic pathways by:
Suppressing transforming growth factor-β (TGF-β)
Limiting mesangial matrix expansion
Preserving nephron mass⁹¹⁰
Vitamin D deficiency removes these inhibitory signals, leading to:
Tubulointerstitial fibrosis
Mesangial expansion
Irreversible nephron loss
Once fibrosis is established, recovery of renal structure is unlikely, making early hormonal correction clinically meaningful¹¹ (see Figure 3).
Secondary Hyperparathyroidism: A Chronic Renal Stressor
Low vitamin D impairs intestinal calcium absorption, triggering compensatory increases in parathyroid hormone (PTH).
Chronic secondary hyperparathyroidism results in:
Phosphate retention
Increased renal oxygen demand
Vascular and renal calcification
Tubular injury and oxidative stress¹²¹³
This process is frequently present early in kidney dysfunction, well before advanced chronic kidney disease is diagnosed, and is often missed when PTH and phosphate trends are not assessed (see Figure 2).
Inflammation, Immunity, and Renal Injury
The kidneys are immunologically active organs. Vitamin D modulates innate and adaptive immunity by:
Reducing pro-inflammatory cytokine production
Supporting regulatory T-cell activity
Protecting podocytes from immune-mediated injury¹⁴¹⁵
Low vitamin D levels are associated with increased oxidative stress, endothelial dysfunction, and worse outcomes in diabetic nephropathy, hypertensive kidney disease, IgA nephropathy, and lupus nephritis¹⁶¹⁷.
Proteinuria and Podocyte Integrity
Proteinuria is not merely a marker of kidney disease—it is directly nephrotoxic.
Vitamin D supports:
Podocyte cytoskeletal stability
Slit diaphragm integrity
Glomerular basement membrane function¹⁸
Vitamin D deficiency is associated with increased albuminuria, faster eGFR decline, and higher cardiovascular mortality in patients with chronic kidney disease¹⁹²⁰.
Why This Relationship Is Commonly Missed

Standard kidney evaluations rely on late markers:
Serum creatinine
eGFR
Basic urinalysis
What is often omitted:
Contextual interpretation of vitamin D levels
Early PTH assessment
Phosphate trends
Recognition of vitamin D as a renal hormone
As a result, endocrine-driven renal stress may persist for years before irreversible structural damage becomes evident.
Bottom Line
Vitamin D is a kidney-activated hormone essential for maintaining renal stability. When vitamin D levels are low, the kidneys are exposed to increased pressure, inflammation, fibrosis, and hormonal stress long before traditional labs reveal overt disease. Identifying and correcting vitamin D deficiency represents a meaningful opportunity to preserve long-term kidney health.
Ready to Look Deeper?
🩺 Concerned about kidney function, vitamin D status, or unexplained lab trends? A comprehensive, physiology-driven evaluation can often identify problems years before irreversible kidney damage occurs.
👉 Become a Patient – Stages of Life Medical Institute
References
Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357(3):266-281.https://pubmed.ncbi.nlm.nih.gov/17634462/
Levin A, et al. Vitamin D, kidney disease, and mortality. Kidney Int. 2007;71(1):31-38.https://pubmed.ncbi.nlm.nih.gov/17051152/
Christakos S, et al. Vitamin D metabolism. Endocrinol Metab Clin North Am. 2010;39(2):243-253.https://pubmed.ncbi.nlm.nih.gov/20511049/
Dusso AS, Brown AJ, Slatopolsky E. Vitamin D. Am J Physiol Renal Physiol. 2005;289:F8-F28.https://pubmed.ncbi.nlm.nih.gov/15951480/
Shimada T, et al. FGF-23 and vitamin D regulation. J Bone Miner Res. 2004;19(3):429-435.https://pubmed.ncbi.nlm.nih.gov/15040831/
Li YC, et al. Vitamin D suppresses renin. J Clin Invest. 2002;110(2):229-238.https://pubmed.ncbi.nlm.nih.gov/12122115/
Forman JP, et al. Vitamin D deficiency and hypertension. Hypertension. 2007;49(5):1063-1069.https://pubmed.ncbi.nlm.nih.gov/17372031/
de Boer IH, et al. Vitamin D and albuminuria. Clin J Am Soc Nephrol. 2010;5(5):890-898.https://pubmed.ncbi.nlm.nih.gov/20378825/
Tan X, et al. Vitamin D and renal fibrosis. Kidney Int. 2006;70(12):2075-2085.https://pubmed.ncbi.nlm.nih.gov/17035934/
Zhang Z, et al. Vitamin D receptor activation and kidney fibrosis. J Am Soc Nephrol. 2010;21(12):2098-2109.https://pubmed.ncbi.nlm.nih.gov/20966126/
Eddy AA. Progression of chronic kidney disease. Adv Chronic Kidney Dis. 2005;12(4):353-365.https://pubmed.ncbi.nlm.nih.gov/16198273/
Slatopolsky E, et al. Pathogenesis of secondary hyperparathyroidism. Kidney Int. 2003;63(Suppl 85):S14-S19.https://pubmed.ncbi.nlm.nih.gov/12753294/
Goodman WG, et al. Vascular calcification in CKD. N Engl J Med. 2000;342(20):1478-1483.https://pubmed.ncbi.nlm.nih.gov/10816185/
Liu PT, et al. Vitamin D and innate immunity. Nat Rev Immunol. 2008;8(5):341-352.https://pubmed.ncbi.nlm.nih.gov/18437166/
Mora JR, et al. Vitamin D and immune regulation. Nat Rev Immunol. 2008;8(9):685-698.https://pubmed.ncbi.nlm.nih.gov/18787518/
Pilz S, et al. Vitamin D and cardiovascular-renal risk. Nutrients. 2013;5(10):4179-4194.https://pubmed.ncbi.nlm.nih.gov/24158433/
Melamed ML, et al. Vitamin D and mortality in CKD. Arch Intern Med. 2008;168(15):1629-1637.https://pubmed.ncbi.nlm.nih.gov/18695076/
Kuhlmann A, et al. Vitamin D receptor in podocytes. J Am Soc Nephrol. 2004;15(4):864-873.https://pubmed.ncbi.nlm.nih.gov/15034092/
Ravani P, et al. Vitamin D and proteinuria. Clin J Am Soc Nephrol. 2009;4(5):872-878.https://pubmed.ncbi.nlm.nih.gov/19339421/
Drechsler C, et al. Vitamin D deficiency and outcomes in CKD. Kidney Int. 2010;77(4):348-354.https://pubmed.ncbi.nlm.nih.gov/20032965/
The medical references cited in this article are provided for educational purposes only and are intended to support general scientific discussion. They are not a substitute for individualized medical advice, diagnosis, or treatment. Clinical decisions should always be made in consultation with a qualified healthcare professional who can account for a patient’s unique medical history, medications, and circumstances.


1917 Boothe Circle, Suite 171
Longwood, Florida 32750
Tel: 407-679-3337
Fax: 407-678-7246




.webp)