

Influenza Is Rising — COVID Is Still Circulating. Test Frequently
- David S. Klein, MD FACA FACPM

- Jan 5
- 4 min read
Be Prepared. Test Early. Treat Promptly.
We are seeing a clear seasonal uptick in influenza, particularly Influenza A, with Influenza B beginning to follow—an expected epidemiologic pattern as respiratory virus season accelerates¹⁷.
At the same time, COVID-19 continues to circulate, often presenting with symptoms indistinguishable from influenza in the early phase²⁸. Clinically, this overlap increases the risk of delayed testing and missed treatment windows, particularly for influenza where antiviral therapy is time-sensitive¹².
This is not a message of alarm—it is a message of preparation.

Influenza and COVID-19 frequently present with overlapping symptoms, especially in the first 24–72 hours³¹¹:
Fever or chills
Headache and body aches
Fatigue
Sore throat
Cough or chest tightness
Because treatment strategies differ, identifying the causative virus matters—particularly during the first 48 hours of illness, when antiviral therapy for influenza is most effective¹²⁶.
At-Home Testing: Essential This Season

Every household should keep combined at-home influenza and COVID-19 rapid tests available before symptoms begin⁸¹³. My advice is to get several boxes, as you will likely be testing yourself more than once.
Testing should occur immediately at symptom onset, not after several days of illness:
Positive for influenza → antiviral therapy may be indicated¹²
Positive for COVID-19 → supportive care and risk-based treatment decisions
Negative but symptomatic → repeat testing in 24 hours if symptoms persist⁸
Early testing is the gateway to effective treatment and complication reduction¹⁴.
Influenza vaccination remains a reasonable preventive strategy, particularly for adults over 50 and those with chronic medical conditions¹⁵.
As with COVID vaccination, immunity is not absolute and does not reliably prevent infection. Its primary benefit is reduction in disease severity, hospitalization, and complications, not sterilizing immunity¹⁵.
Where Exposure Risk Is Highest
Transmission risk increases substantially in enclosed, high-density environments⁷¹¹:
Airports and airplanes
Crowded indoor venues
Schools and households with children
Social gatherings during peak season
There is no practical way to eliminate exposure—only to manage risk intelligently.
What Actually Helps Prevent Infection
Hand Hygiene
Frequent handwashing remains one of the most effective defenses against both influenza and COVID-19, reducing contact transmission from contaminated surfaces⁷.
Masks
Masks are situational and a matter of personal choice. Their greatest benefit may be behavioral reinforcement in high-risk environments rather than absolute protection.
Eating Out
Prefer hot foods and hot beverages
Avoid shared utensils or drinking vessels
Use caution with cold or uncooked foods
What to Have on Hand — Before You Get Sick
Early treatment gives the best result. Having these products on hand is like having a fire extinguisher handy, in case of fire.
Over-the-Counter Support
N-Acetylcysteine (NAC) — 500 mg, four times daily
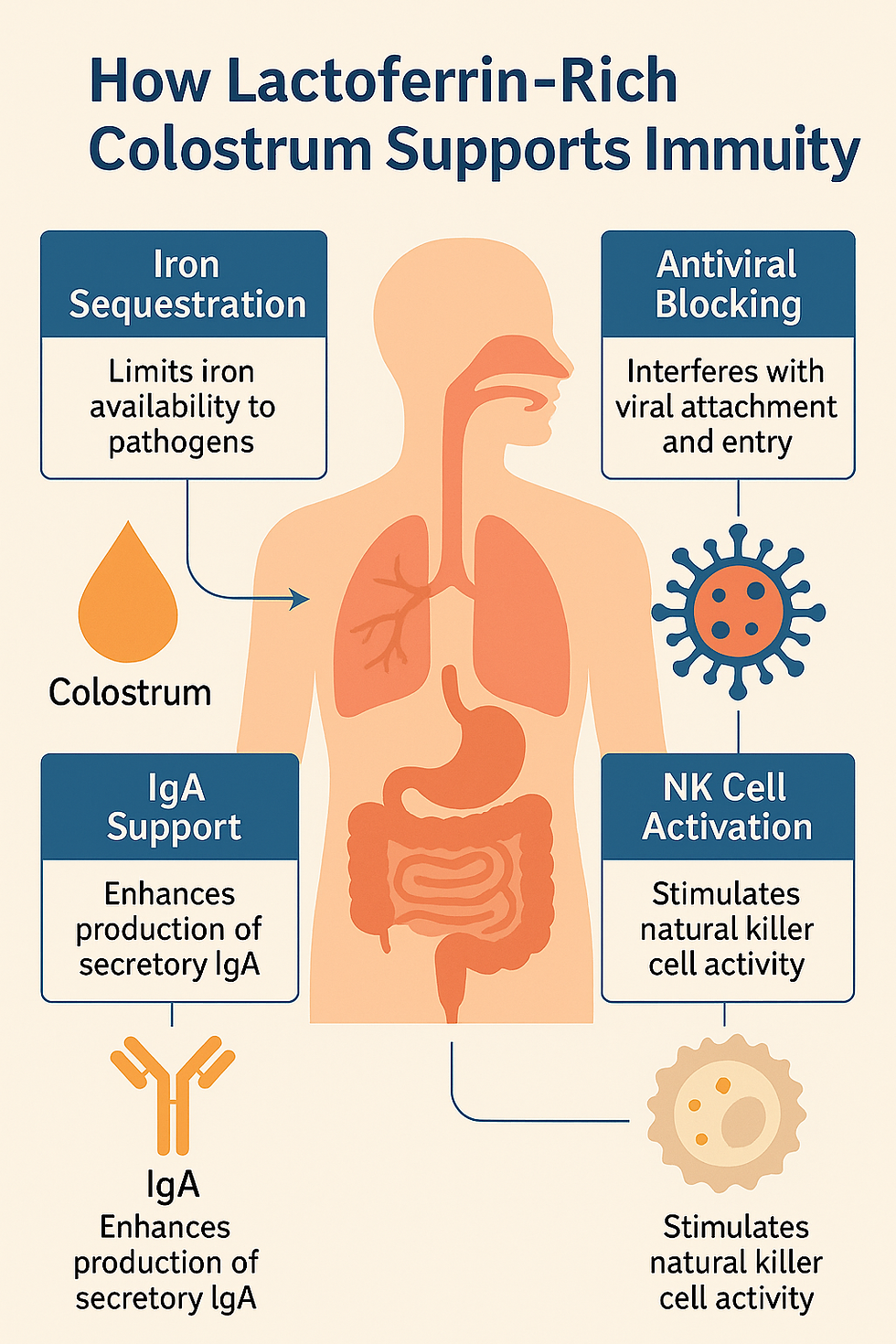
Lactoferrin-containing colostrum — two capsules, four times daily
These agents support mucus clearance, oxidative balance, and immune modulation, and appear most effective when initiated early in viral illness⁹¹⁰.

When Tamiflu Works Best
Oseltamivir demonstrates its greatest clinical benefit when started within 48 hours of symptom onset¹²⁶. After this window, benefit diminishes but may still be considered in higher-risk patients⁴.
Standard Adult Dosing
75 mg by mouth, twice daily for 5 days¹²
Who Benefits Most
Adults over 50
Patients with chronic cardiopulmonary, metabolic, or immune conditions
Individuals with significant fever, myalgias, or rapid clinical decline⁴⁹
Tamiflu does not cure influenza, but it can shorten illness duration, reduce symptom severity, and lower complication risk when used appropriately¹⁴.
COVID-19 Treatment Considerations
COVID-19 management remains individualized. Many patients require only supportive care, while higher-risk individuals may benefit from additional therapy²⁸.
Vaccination status does not eliminate infection risk, and severity—not mere positivity—defines clinical concern².
Final Takeaway
This is influenza season, and COVID-19 remains present.
Test early
Treat promptly
Prepare in advance
Avoid delay and denial
Prepared patients consistently fare better than reactive ones.
References
Uyeki TM, et al. Clinical Practice Guidelines for the Diagnosis and Treatment of Influenza. Clin Infect Dis. 2019;68(6):e1–e47. doi:10.1093/cid/ciy866
Centers for Disease Control and Prevention. Influenza Antiviral Medications: Summary for Clinicians. Updated 2024.
Treanor JJ. Influenza Viruses, Including Avian Influenza and Swine Influenza. N Engl J Med. 2005;353:1574–1585. doi:10.1056/NEJMra052639
Muthuri SG, et al. Effectiveness of Neuraminidase Inhibitors in Reducing Mortality in Influenza. Lancet Respir Med. 2014;2(5):395–404. doi:10.1016/S2213-2600(14)70041-4
Jefferson T, et al. Neuraminidase Inhibitors for Preventing and Treating Influenza. Cochrane Database Syst Rev. 2014;4:CD008965.
Hayden FG, et al. Use of the Neuraminidase Inhibitor Oseltamivir in Experimental Human Influenza. JAMA. 1999;282(13):1240–1246. doi:10.1001/jama.282.13.1240
World Health Organization. Influenza (Seasonal): Fact Sheet. Updated 2024.
Centers for Disease Control and Prevention. Overview of Testing for SARS-CoV-2 and Influenza Viruses. Updated 2024.
Butler CC, et al. Effect of Antiviral Treatment on Influenza Symptoms and Complications. BMJ. 2020;368:l6985.
Fiore AE, et al. Antiviral Agents for the Treatment and Chemoprophylaxis of Influenza. MMWR Recomm Rep. 2011;60(RR-1):1–24.
Taubenberger JK, Morens DM. The Pathology of Influenza Virus Infections. Annu Rev Pathol. 2008;3:499–522.
Uyeki TM. Influenza. Ann Intern Med. 2017;167(5):ITC33–ITC48.
Peeling RW, et al. Diagnostics for COVID-19: Rapid Tests and Their Role. Lancet Infect Dis. 2022;22(5):e1–e12.
Brendish NJ, et al. Impact of Point-of-Care Testing for Respiratory Viruses. Lancet Respir Med. 2017;5(5):401–411.
Nichol KL, et al. Influenza Vaccination and Reduction in Hospitalization and Death. N Engl J Med. 2003;348:1322–1332.
This article is for educational purposes only and is not intended as a substitute for individualized medical advice, diagnosis, or treatment. Medication decisions should be made in consultation with a licensed healthcare professional, based on individual medical history and risk factors.


1917 Boothe Circle, Suite 171
Longwood, Florida 32750
Tel: 407-679-3337
Fax: 407-678-7246



.webp)